
Why has HSS invested in building it's own systems?
The work that determines whether an EPR programme succeeds, mapping and training thousands of staff, coordinating go lives across sites, building a safe EPMA configuration, is usually held together by spreadsheets, email and a learning management system stretched well beyond what it was designed for. This holds until the programme comes under real pressure, and it is precisely this work that fails first: the version nobody can find, the task everyone assumed someone else had done, the sign-off that cannot be evidenced when it matters most.
HSS builds that work into purpose built systems instead, so the right way of doing it becomes simply the way the system works and the expertise sits in the system rather than only in the people. Some of these systems open up ways of running a programme that were not previously possible, such as a go live staffed by your own people rather than external floorwalkers, or training booked across thousands of staff at a pace manual methods cannot reach. Others take a single high-stakes task, where a coordination failure becomes a clinical safety or governance problem, and make it provable from end to end.
Explore our custom products
TAIC - Go live support, intelligently coordinated
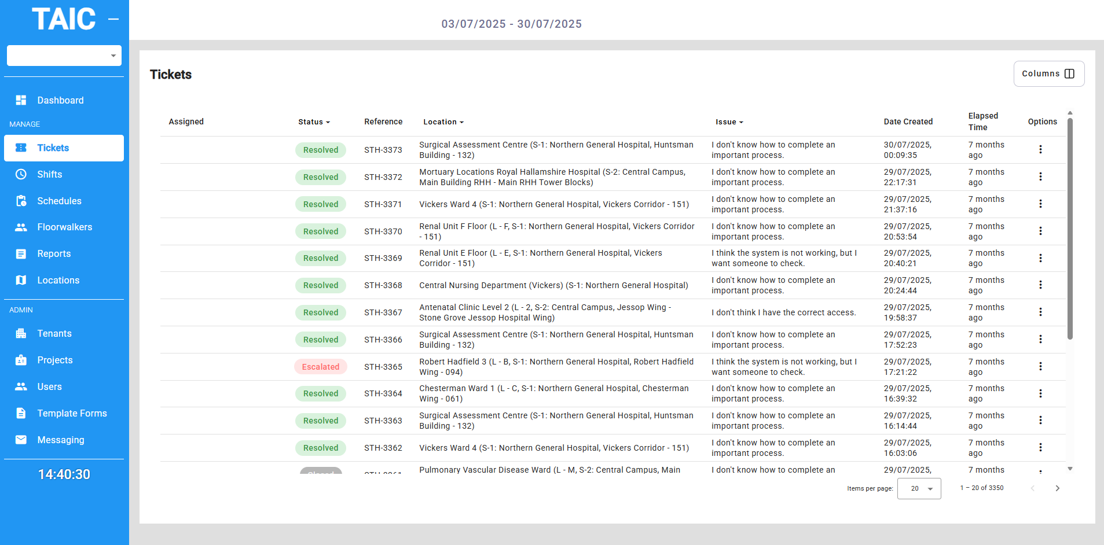
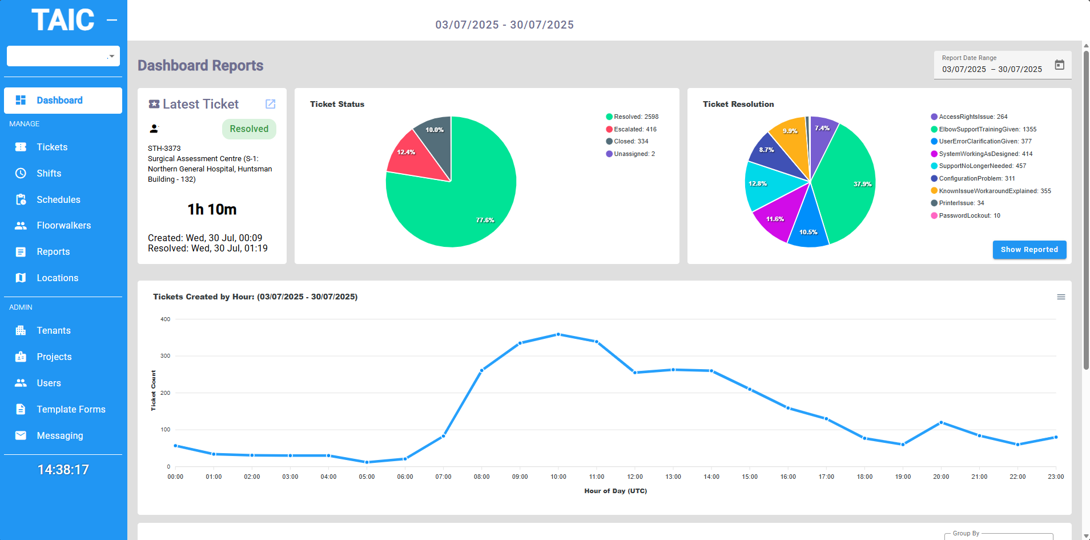
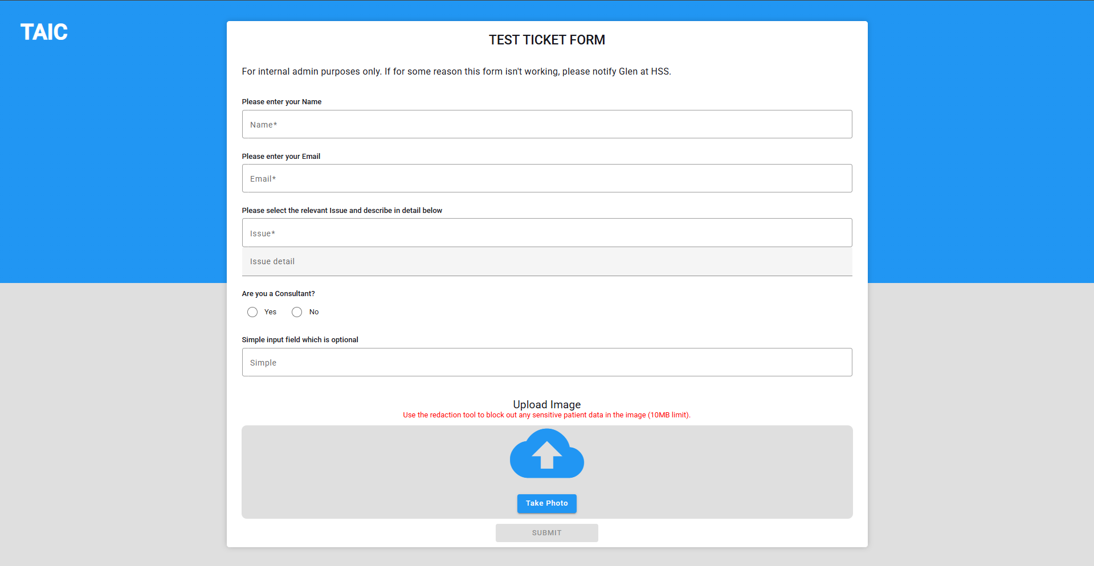
At the height of a go-live, support has to reach the right ward at the right moment across multiple sites, while command needs a live picture to make decisions. Run on phones, radios and messaging, that coordination breaks under volume, and the traditional answer, enough external floorwalkers that someone is always within sight, can cost upward of £500,000 on a large go-live. TAIC routes each support request to the nearest available person with the right system knowledge, so coverage depends on response capacity rather than proximity, and a Trust with a trained super user or navigator network can run its go-live on its own people. Command sees ticket volumes, staff locations and emerging issues live on one screen, resolvable requests stay off the central helpdesk, and the data captured becomes the post-go-live report leadership needs for the board.
TMA - Training Mapping Analysis (and booking)
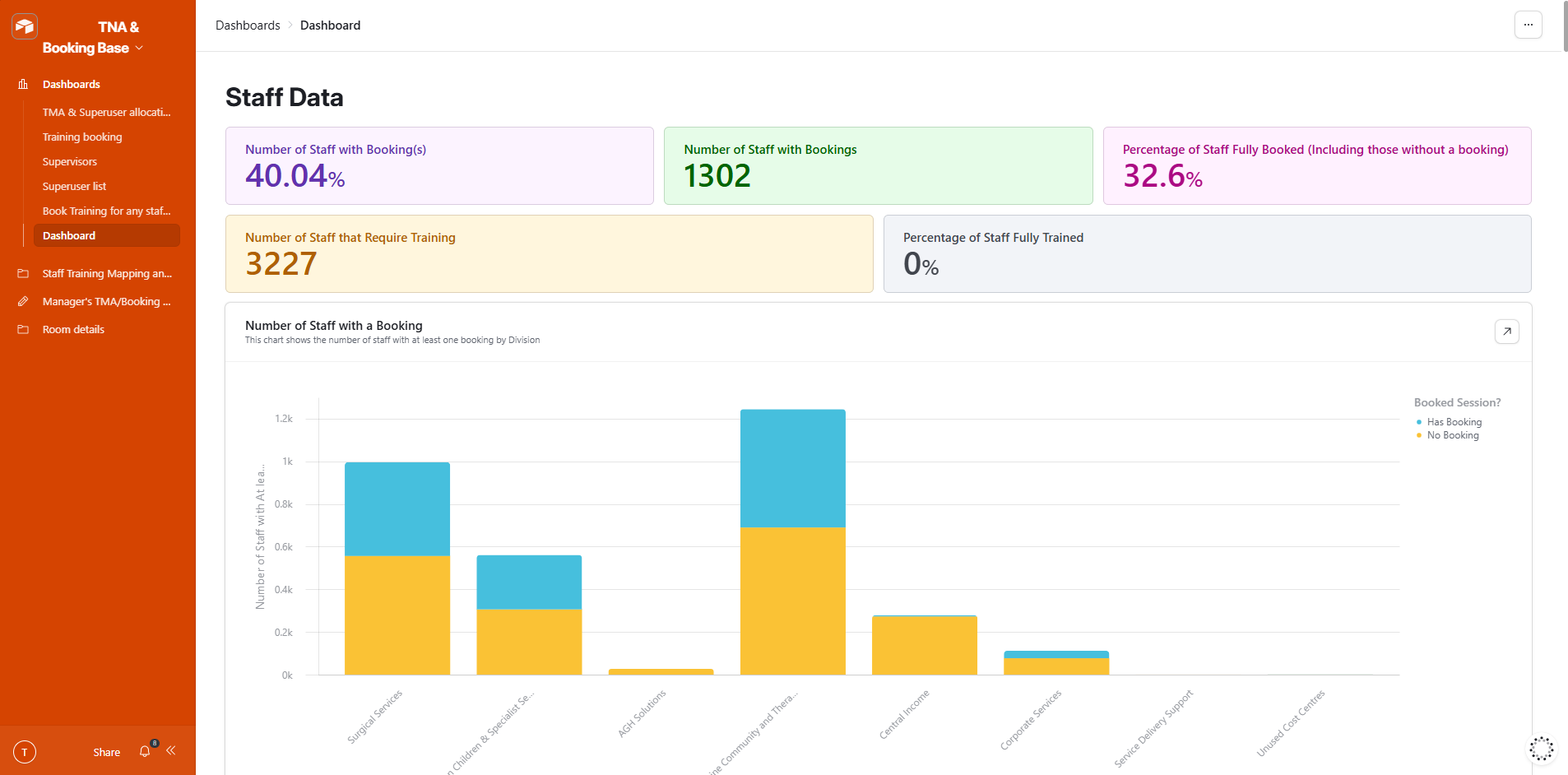
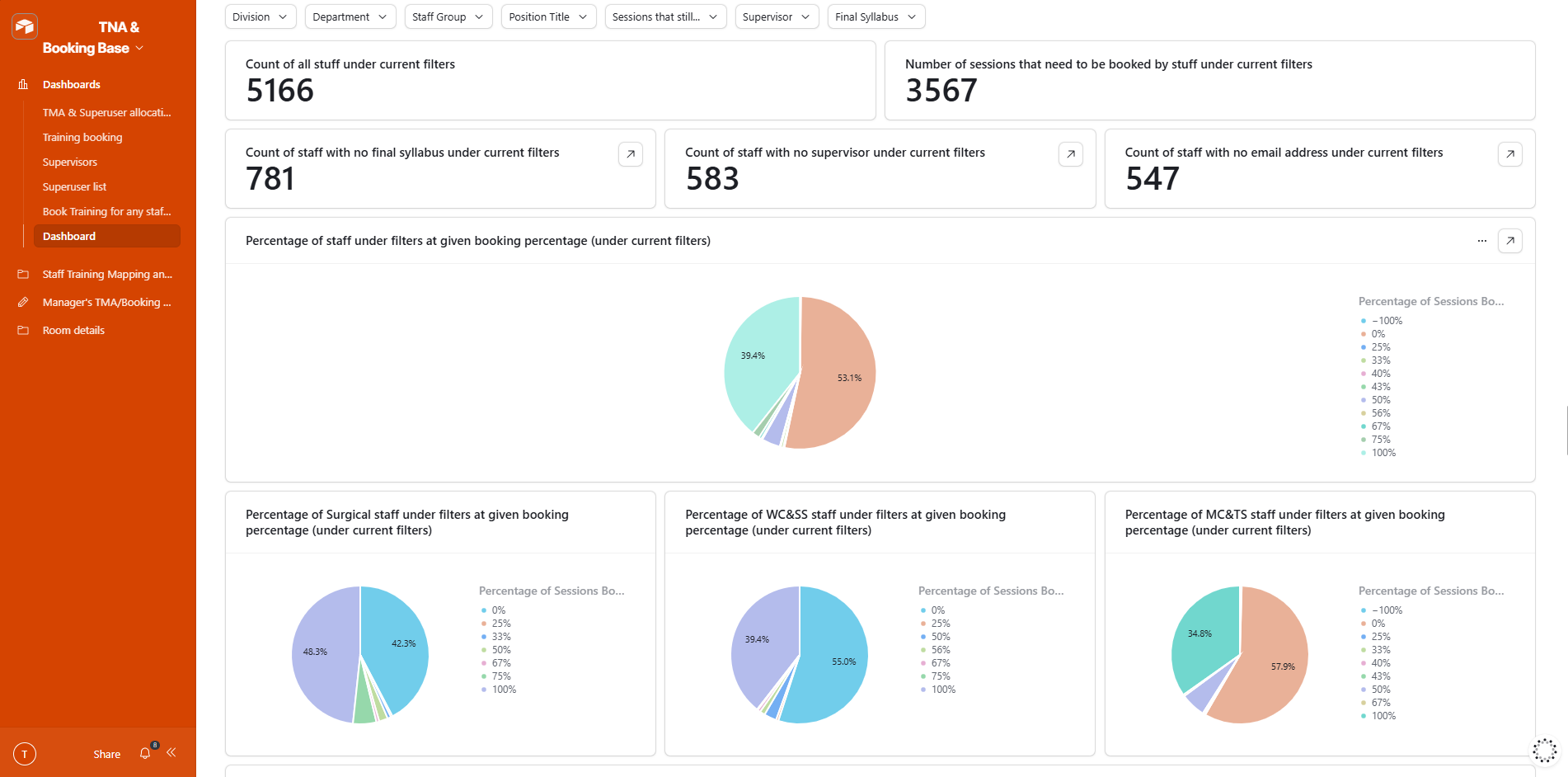
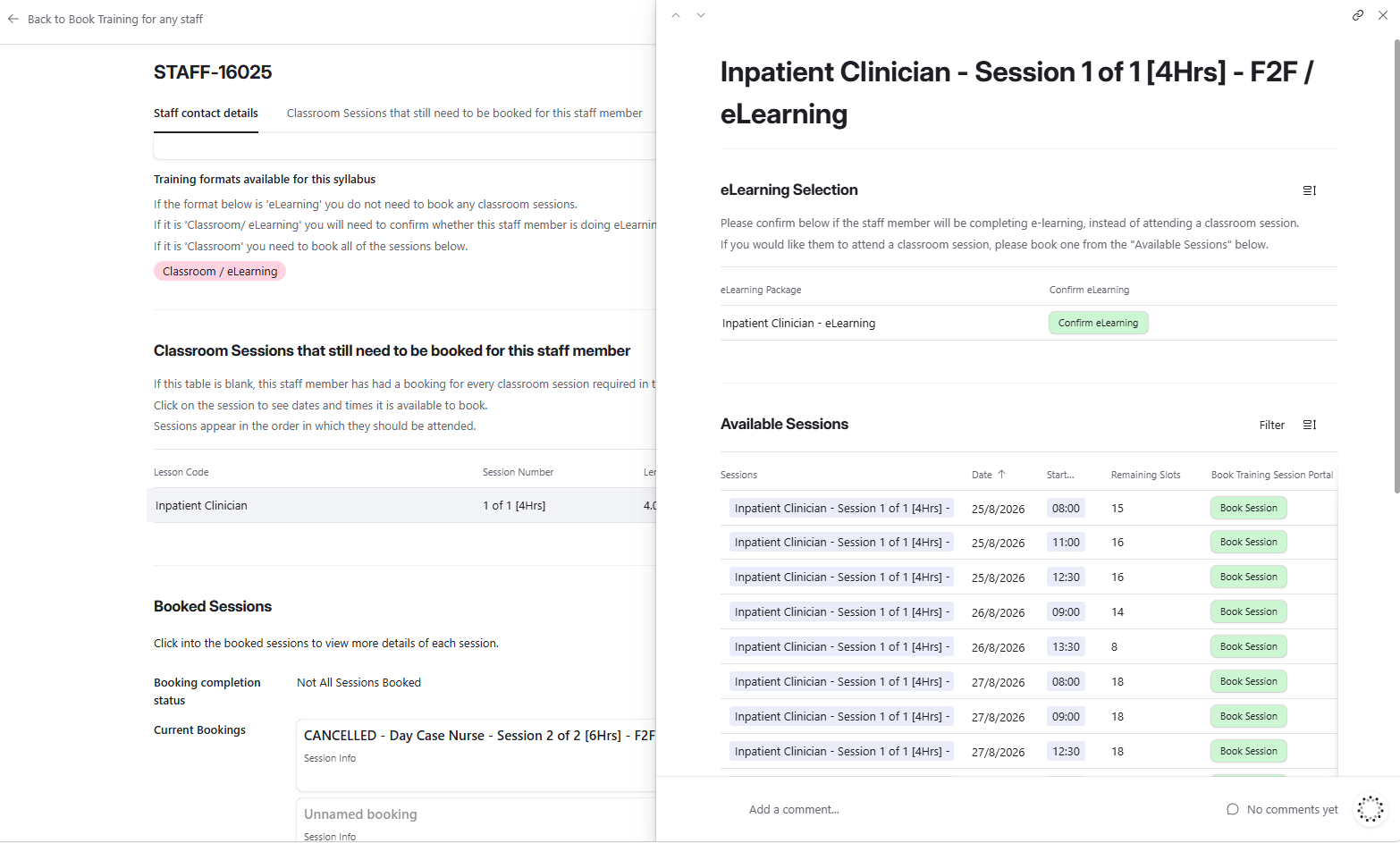
An EPR go-live means training thousands of staff, in the right course for their role, inside a window of weeks. The usual mix of ESR extracts, departmental spreadsheets and a steady-state LMS cannot reliably show who has been booked onto what until the gaps are too wide to close, and staff who reach go-live undertrained are both a patient safety risk and a reason for the supplier and NHS England to press for a later date. TMA maps each member of staff to the right training, lets their supervisor book them through a simple self-service interface, and gives programme leadership live compliance data in time to act on it. At two London acute trusts, that visibility let senior clinical leaders target the departments falling behind, and attendance compliance rose from 68 per cent to over 90 per cent.
TDMS -Training Development Management System

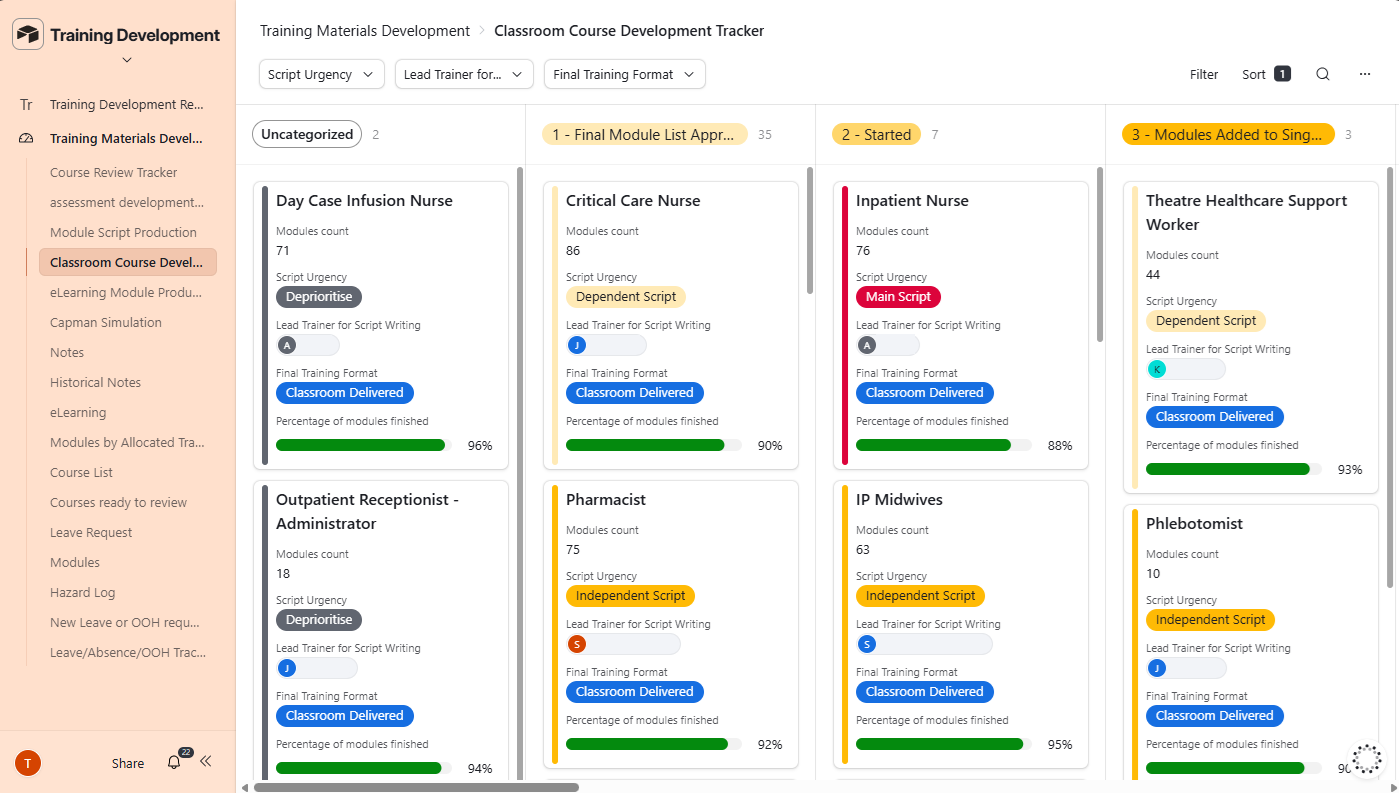
Producing the training content for a go-live is a large writing project: several hundred module scripts, assembled into dozens of role-specific courses, each signed off against the Trust's clinical safety obligations, inside a fixed window. Coordinated through shared drives, email and spreadsheets, modules fall silently out of date, courses are built from scripts that were later revised, and a hazard recorded as "mitigated by training" cannot be traced to the content and staff that actually address it. TDMS holds every module, course, sign-off and hazard link in one place, with each change recorded against the person who made it, so the line from a clinical risk to the trained staff who mitigate it is documented end to end. Because the system carries the coordination, senior trainers spend their time on the work only they can do, the SME and workstream relationships and the quality of the content, rather than on keeping a tracker current. It was built to hold under pressure: we used it to recover a large acute trust's programme after a previous supplier had been unable to deliver, producing over 400 scripts, 94 classroom courses and more than 240 eLearning modules in time for the planned go-live.
PBMS - Pharmacy Build and Management System
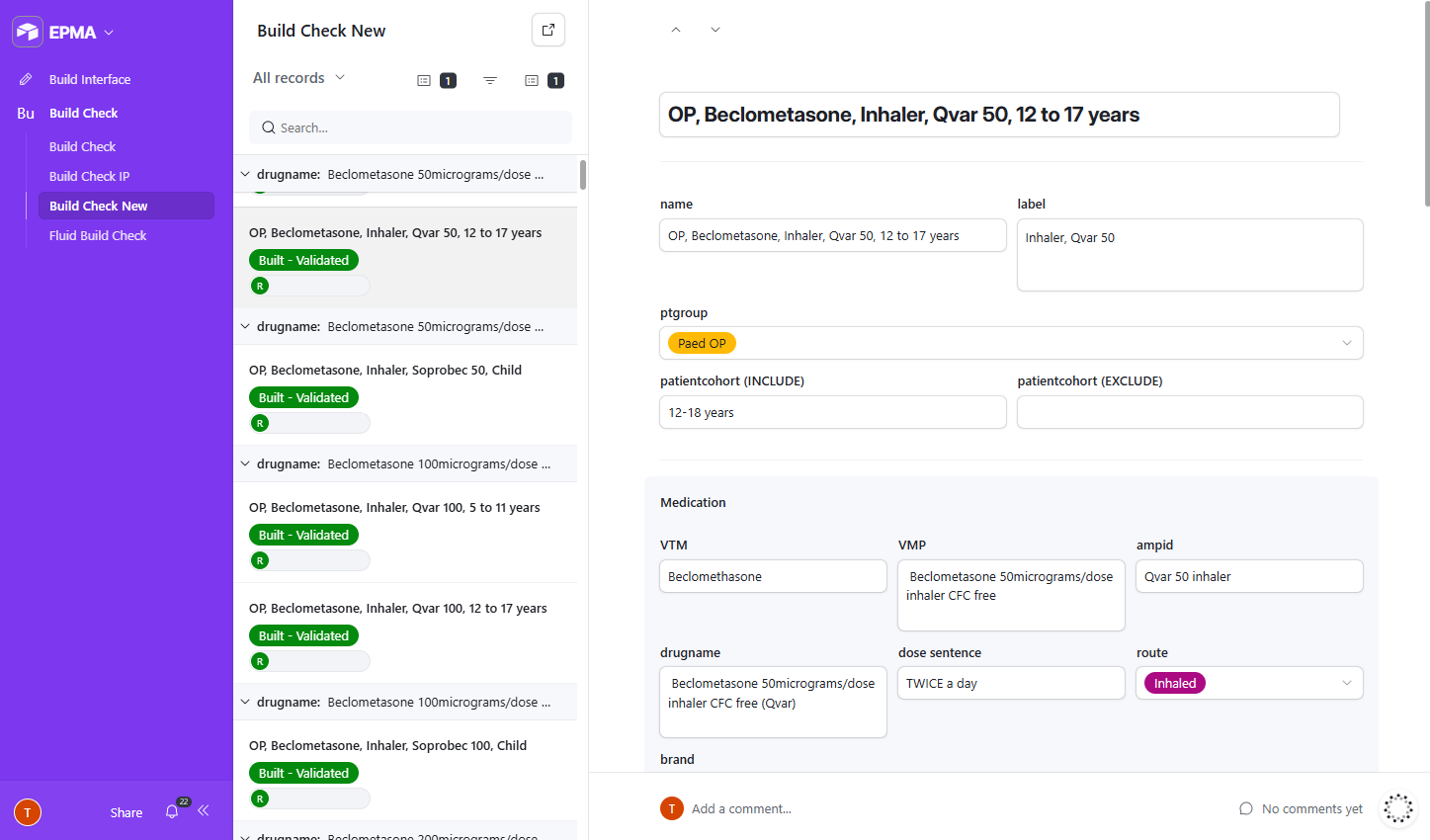
Configuring an EPMA system is months of structured data entry, clinical validation and sign-off across pharmacy, clinical, digital and safety teams, with every drug, dose range and rule needing to be entered, checked and confirmed safe before go-live. Run on shared spreadsheets, the configuration that reaches the live system may not match what anyone agreed, with no record of what was entered, by whom, or whether it was later changed, a risk that becomes acute in paediatric prescribing, where dose ranges are weight and age dependent. PBMS structures the build into discrete validation stages, holds the definitive record of every entry with a complete and unalterable history, and links each configuration record to the clinical safety hazard it mitigates. HSS and Trust staff work in the same system at once, each in the view relevant to their role, which produces the DCB0129 clinical safety evidence as a natural output of the build rather than a document assembled afterwards. It was proven first on a paediatric EPMA build, the most demanding context the approach could be tested in.